Independent Medical Review is probably the most contentious change introduced to the California workers' compensation system in history because it upends, in dramatic fashion, The Culture.
Over the course of a hundred years physicians had sought, and were granted, great latitude to order up pretty much any "treatment" desired for an injured worker, and frankly there were many that abused this privilege.
Doctor's orders were sacrosanct - for instance, I recall when practicing law many cases where the physician ordered up a new, specific mattress, regardless of the cost and regardless of less costly alternatives, and the carrier/employer would be obligated to pay for it.
Any objection to such orders were stymied at the workers' compensation judge level because, the reasoning went, if the doctor ordered it then it must be necessary. After all, I wasn't a doctor, the claims adjuster wasn't a doctor, the judge wasn't a doctor. It didn't matter that the physician didn't have any evidence of treatment efficacy - he or she is a doctor!
There was a period of time when chiropractors ran amok, and it wasn't unusual to see "treatment" consisting of chiropractic adjustments and massage every week for years regardless of what published treatment guidelines said.
Again, objections to such over treatment abuse was stifled at the hearing level because doctor's orders trumped everything. A hard cap on chiropractic visits put the issue to rest eventually and survived judicial scrutiny and constitutional challenge.
There are many, many such examples where the medical profession's elevated status cleared the path for the provision of "treatment" that would not be tolerated in any other medical setting.
Guidelines didn't change that culture, push back from carriers/employers didn't change that behavior, Utilization Review didn't make much of a difference. The Culture remained - if a doctor ordered something called "treatment" then the carrier/employer was obliged to provide it.
It's very difficult to effect change to The Culture.
 |
| This is my preferred Culture. |
Culture means a practice is deeply embedded and accepted by a large population.
If you're absolutely truthful with yourself, you'll agree that The Culture of medical treatment in workers' compensation had taken on preposterous qualities.
That's why we have IMR now - frankly because the people that could not behave themselves took it too far, for one reason or the other.
It's a huge, radical shift and resulted in a revolution. New rules, new mandates, new systems - old expectations, old operations, old sentiment: a confluence of mixed emotions seeking to either vilify or justify this new process.
And this is not to say that there are injured workers who are not getting medical treatment that they otherwise should be getting - because there are many case examples where reasonable doctor's orders aren't being granted now - a very public example is when
Comp Laude Award winner
Dwight Johnson, a double amputee, was denied handicapped modifications to his restroom so he didn't have to travel to the municipal gymnasium just to take a shower.
Those were doctor's orders that were initially denied in UR, but ultimately provided after a change in adjuster, a lawyer, and more well written orders from the doctor.
Late Friday afternoon the California Department of Industrial Relations released
the first report on the IMR system, and declared it a success. Whether one agrees with that conclusion is dependent on your personal position relative to SB 863, of course.
And I'm not going to pass judgment at this time on whether IMR is a success or not, but there are some very interesting
observations made in the report.
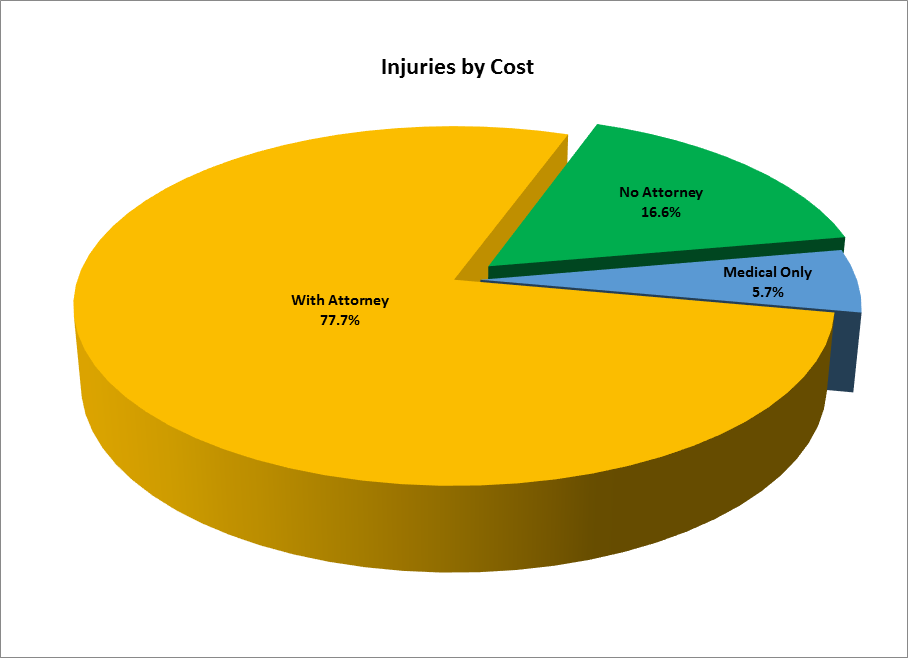
For instance, it seems that an unrepresented injured worker is more likely to succeed in an IMR review than one with attorney representation, albeit by a small margin.
And where additional consultation or diagnostic testing is involved, IMR overturns the UR denial over a third of the time.
Nearly half of all IMR requests involves pharmaceuticals, and most of those involve opioids. I would expect those numbers to ameliorate over time, bowing to the next medical trend that hits work comp.
Indicating to me an acceptance of restrictions in medical practice via treatment guidelines, the report says that UR was overturned more often by IMR in cases where date of injury was 2013. UR in earlier cases was more often upheld.
You certainly can draw your own conclusions from DIR's report, but I think DWC is correct in its analysis regarding the high rate of IMR upholding UR:
"Our analysis highlights two reasons for the comparatively high uphold rate in the DWC IMR program. First, disputed treatment requests that were not consistent with evidence-based guidelines were highly likely to be overturned. Additionally, medical records for IMR FDLs that upheld UR decisions frequently did not contain adequate documentation to justify medical necessity."
To state it more
succinctly: doctors don't practice evidence based medicine and records aren't getting to reviewers.
Both are real problems. Docs that aren't following guidelines, or offering alternative evidence aren't doing their jobs. And we've all heard many anecdotes of records not making it to reviewers either intentionally or through gross negligence.
The real legal question of course is whether injured workers are getting the medical care that is guaranteed them via the state Constitution: "full provision for such medical, surgical, hospital and other remedial treatment as is requisite to cure and relieve from the effects of such injury."
The word "requisite" means necessary. This is tied to "cure and relieve." For many years this concept expanded, as noted above, to include many items that may not actually be medical, or even "other remedial" treatment, but the stated public policy of the state's workers' compensation laws were that they be liberally construed in favor of the injured worker. So if a doctor said it was necessary then it was...
Now, the First District Court of Appeals for California
has agreed to hear a constitutional challenge to the IMR process.
A date and time for the oral argument in
Stevens v. WCAB, No. A143043, has not yet been set. Briefing in the matter is set to wrap up next Monday.
All of the usual players have
weighed in with predictable arguments: California Applicants' Attorneys Association, Division of Workers' Compensation, California Workers' Compensation Institute, Property and Casualty Insurers Association of America, California Chamber of Commerce, and of course defendant State Compensation Insurance Fund.
This is the second time the case has gone to the appellate court. The first time it was kicked back for failure to exhaust administrative remedies. Those remedies have now run the course.
Appellant's
argument is that the IMR procedure codified in Labor Code Section 4610.6 violates the state constitution because of the anonymity of the decision-maker and the limited ability of an aggrieved party to appeal the decision reached.
Injured worker Stevens tripped over an area rug and fell while carrying boxes of magazines while at work in 1997. She suffered a broken foot, but her recovery did not go smoothly.
Through the years, Stevens has undergone numerous surgeries and is now confined to a wheelchair. The combination of her chronic pain and lack of mobility has left her struggling with depression and unable to work.
In 2013, a workers' compensation judge declared her to be permanently and totally disabled. Following this decision, her doctor recommended she receive medication management and home health care assistance.
SCIF submitted the doctor's recommendations to utilization review and then denied authorization for the requested services.
Maximus Federal Services, the contractor providing IMR services to the workers’ compensation system, affirmed that decision in February.
DWC,
in its report, says it will continue to maintain IMR program transparency, though their definition of transparency isn't the same as everyone's. But, I do believe that the division is being as transparent as the law permits it to be.
The 1st DCA may have a different idea on transparency.
Regardless, this much is true: liberal interpretation is no longer. Now there must be evidence, and it is reviewed in a stratified manner, with some evidence better than other evidence. That requires doctors, not used to following the rules, to change their practices.
That also requires claims payers to follow the rules and change their practices too - they are responsible for ensuring ALL records (some may not be "relevant") get reviewed.
The Culture change affects everyone, and everyone has to adjust.